

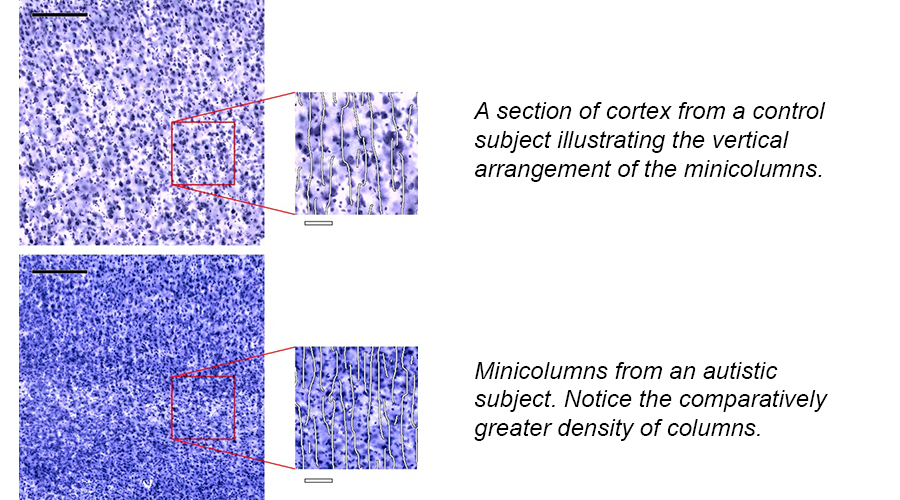
Studies using brain tissues have revealed brain cells in the area called the cerebral cortex are organized in a specific way called “minicolumns”. In people with autism, this organization is different than those without autism. This has led scientists to ask what these columns do and how is it related to autism symptoms?
We asked two of the worlds leading researchers, Steven Chance of Oxford University and Manny Casanova at the University of South Carolina, who have studied the brains of people with autism, to weigh in on this topic. Specifically, we interviewed them to explain how the minicolumnar findings have impacted the field of autism research and led to discoveries that are important for families.
So, what is a cortical minicolumn and what do they do?
Steven Chance: There are cells in the cerebral cortex that are arranged in columns. These ‘mini’-columns of cells are typically about one third the width of a human hair. In the typically developed brain, wider minicolumns seem to be associated with processing more individual features of incoming information.
Manny Casanova: Minicolumns are a basic template that is used by neurons to figure out where neurons should go and where they should connect. They also help process the connections of different brain cells. Some people think of minicolumns as the microprocessor of a computer. Indeed, Vernon Mountcastle thoughtof minicolumns as the basic unit of information processing in the brain. More recent experiments have proven that these minicolumns help people to think and to act.
How are they different in people with autism?
Steven Chance: In ASD these minicolumns are between 5% and 10% wider than in those without autism. . This difference may not sound like much, but multiplied over hundreds of thousands of minicolumns throughout the brain it may contribute to a significant difference in brain organization. In addition to cognition and thinking like Manny Casanova pointed out, our lab has recently found these minicolumns in brain areas involved in basic sound and word processing, as well as in areas involved in complex social behavior.
Manny Casanova: Yes, minicolumns affect different aspects of behaviour. We have also found variability in the size of mini columns according to brain area. These changes are consistent with other neuropathological findings and indicate that the minicolumnopathy of autism is part of a process called cortical dysplasia. The presence of cortical dysplasia provides an explanation for intractable seizures and sensory abnormalities commonly observed in ASD. The pathology may be selective as to whom it affects as, on occasion, involved individuals have either a specific genetic or immunological profile.
What does this mean for people with autism?
Steven Chance: The differences in width and spacing of the minicolumns means that they may become too independent and overly focused on individual features in the environment. This may explain the altered cognitive style or focus in many people with autism, and possibly explain the strengths of some people with autism in certain situations.
Manny Casanova: The findings help explain many of the symptoms observed in ASD. We are using the findings to provide new ways for screening for diagnosis, to provide for severity dependent outcome measures that do not rely on behavioral screening, and to introduce a possible therapeutic intervention.
Larger or smaller, what is it?
Steven Chance: The findings depend on the age of the individual. In other words, when the data from studies are compared while accounting for subject age, they suggest that minicolumns are wider in youth in autism but then become narrower in later life. This is interesting because it is consistent across the studies and reinforces tha autism as a developmental condition which changes across the lifespan. It also makes sense in the light of other MRI studies which have shown larger brains in ASD in early life, followed by a loss of this enlargement later on.
Manny Casanova: It may be that the age-related changes in the minicolumnopathy of autism may constitute an adaptive response meant to correct early changes in the cortex; or or it could be the beginning of a neurodegenerative process whose manifestation may appear later on in life. We don’t know, we need more research using brains of people with autism at all ages and abilities.
These questions can only be answered with more brain tissue from individuals across the lifespan. You can help with the discoveries. Register to donate your amazing brain when you don’t need it anymore by going to www.takesbrains.org.

